In this issue of STRIDE we are sharing brief excerpts from the 2021 Australian evidence-based guidelines for diabetes-related foot disease and the companion Diabetes and feet toolkit, to try to encourage as many podiatrists as possible to refer to these resources.
While you may be familiar with these resources, you may not yet be familiar with how the guidelines came about. Firstly, an expert multidisciplinary guideline working group was appointed to develop a guidelines protocol. Secondly, this was followed by the appointment of six multi-disciplinary national panels to enact the protocol and develop one guideline each specifically across six fields:
Adapted from the 2019 International Working Group on the Diabetic Foot (IWGDF) Guidelines on the Prevention and Management of Diabetic Foot Disease, each guideline group included consumer and Aboriginal and Torres Strait Islander Peoples representatives for input on all guideline decisions and considerations. A key focus was the inclusion of implementation considerations in Australia, including specifically for geographically remote and Aboriginal and Torres Strait Islander Peoples.
The methodology used to develop these new guidelines was comprehensive (see page 6 here and page 8 here), and the public consultation process can be learned more about here.
The Diabetes and feet companion toolkit was then designed specifically to help busy multidisciplinary health professionals use guideline-recommended diabetes-related foot disease (DFD) care at any time and place and with the person with a diabetes-related foot ulcer (DFU) right there in front of them. This was funded by the National Diabetes Services Scheme (NDSS), an initiative of the Australian Government and administered by Diabetes Australia, and developed in collaboration with Diabetes Feet Australia and the Australian Diabetes Society.
The goal behind these updated guidelines is to ensure that health professionals in Australia – who care for people with DFD in secondary and tertiary health care settings – have access to consistent up-to-date evidence-based advice; including practical pathways and considerations for the Australian context. These guidelines will now serve as the national multidisciplinary best practice standards of DFD care in Australia and this is why it is so important all podiatrists familiarise themselves with these guidelines.
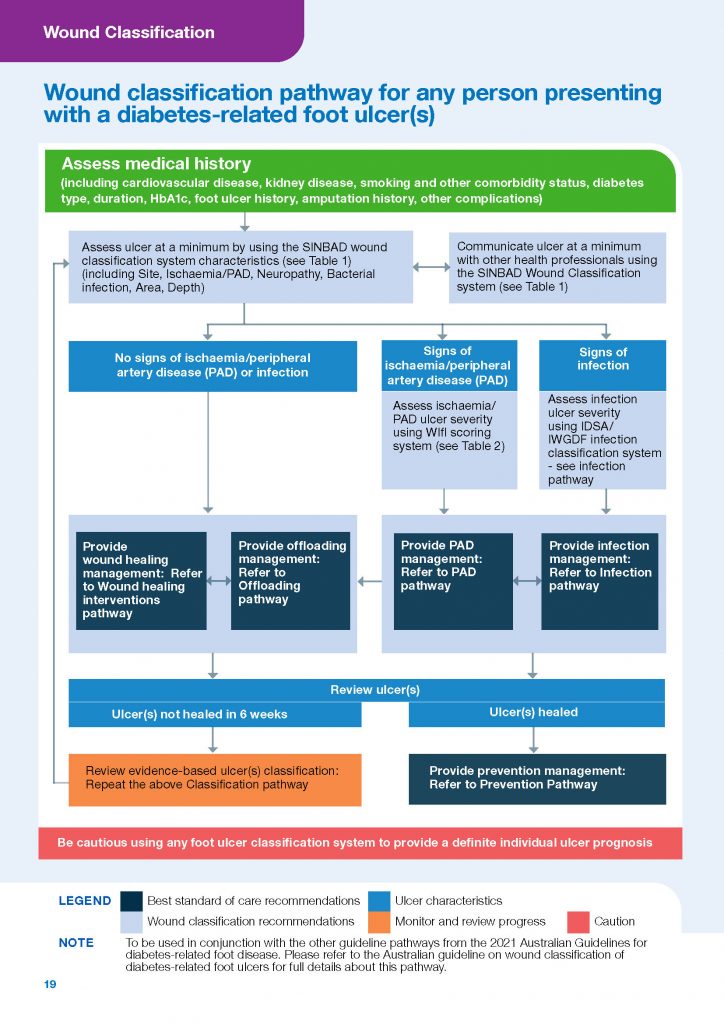
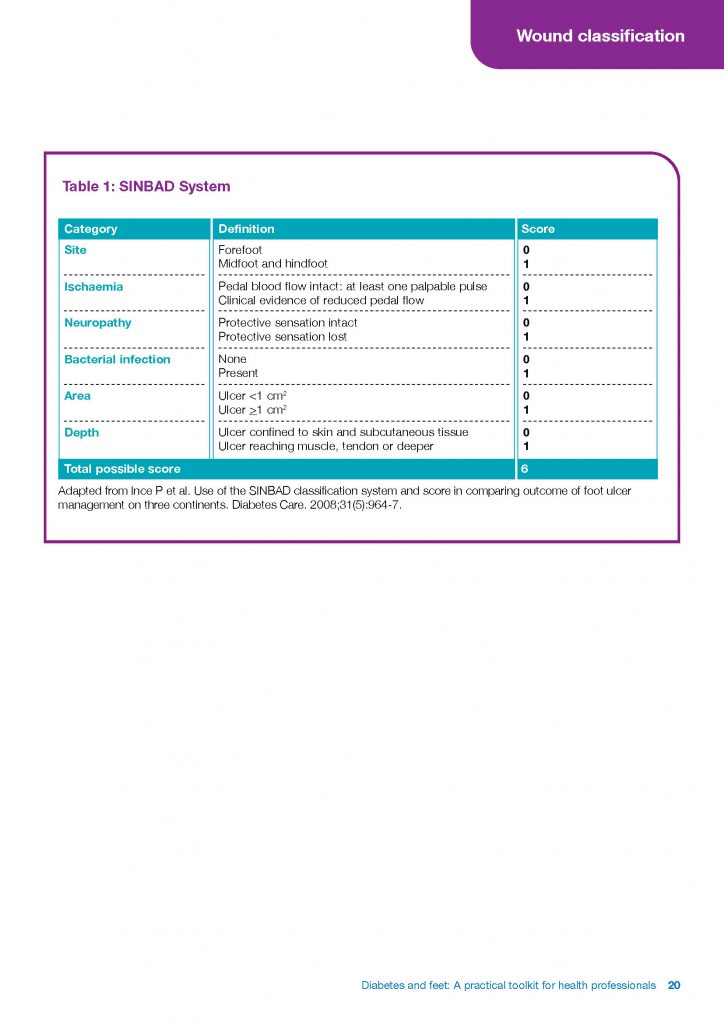
To give you a sense of the information covered in these resources, further below are some excerpts from the Diabetes and feet companion toolkit covering the fields of prevention, wound classification and peripheral artery disease. We encourage you to head here to read the related information in full.
Next month we’ll address the other fields covered which are infection, offloading and wound healing interventions.