Jade's background stems in clinical podiatry with a focus in musculoskeletal health. This is further supported by her clinical research, which has focused on non-surgical interventions for pain management, translating to increased physical activity.
Jade has over five years of experience teaching and developing curriculum within undergraduate podiatry and prosthetic and orthotic courses. The impact of her teaching has been recognised through university dean and vice-chancellor awards.
By John Osborne
John is a podiatrist in private practice in Melbourne, PhD candidate at La Trobe University and recently completed the Certified Sports Podiatrist pathway. If he could have an ideal day it would start with a nice coffee, include some reading and finish with a game of golf.
Let’s first recap on what osteoarthritis is. Osteoarthritis (OA) is a disease of the entire joint complex. It is a result of alterations to joint cartilage, subchondral bone, synovium, the joint capsule, and ligaments. The development of OA is complex, involving a combination of metabolic, mechanical, and inflammatory factors, which lead to damage of the synovial joint and impede its ability to function adequately. It is now known that OA results from an imbalance between joint destruction and joint repair, and is not solely a degenerative disease process1.
Dr Jade Tan shares her experiences on the presentation, diagnosis and treatment of tibiofemoral (TF) and patellofemoral (PF) osteoarthritis, including where the current thinking lies on diagnostic imaging in this regard.
Presentations across the ages
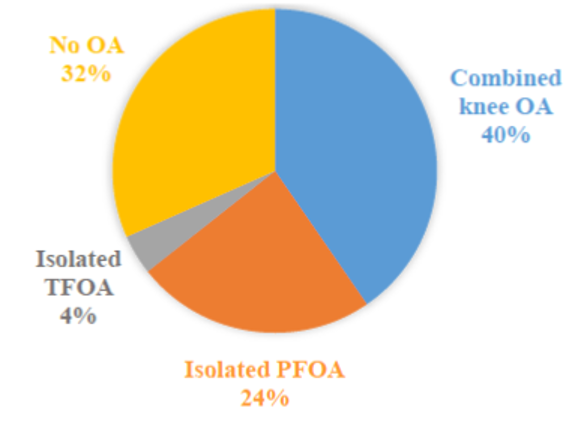
The knee is one of the most common joints in the body to be affected by OA. This is due to the large weight-bearing requirement of the knee. When OA affects the knee, the tibiofemoral (TF) and patellofemoral (PF) joints can be involved. A large proportion (40%) of individuals aged over 50 years with knee pain will present with a combined pattern of knee OA (such as TF and PFOA), with isolated PFOA being the second most common radiographic distribution (24%), and a very small proportion (7%) of individuals presenting with isolated TFOA (4%) (see Figure 1).
Figure 1. Radiographic distribution of knee osteoarthritis in individuals over 50 years with knee pain (modified from Duncan et al.)
Interestingly, incidence and prevalence estimates of knee OA vary depending on the case definition used, with radiographic, symptomatic, and self-reported OA being the most common definitions.
Epidemiology up close
So, how many people in the community have knee OA and PFOA? Interestingly, incidence and prevalence estimates of knee OA vary depending on the case definition used, with radiographic, symptomatic, and self-reported OA being the most common definitions.
Conversely, incidence estimates are less widely reported, reflecting the challenges in conducting prospective studies. Cumulative incidence rates of knee OA range between 6.2 to 27.6%, with the cumulative incidence of isolated TFOA demonstrated to be 5.5% at two years, and further increased to 7.6% at five years. In contrast, the incidence of isolated PFOA has been demonstrated to be 28.8% in the general population over three years. These data demonstrate that the epidemiology of PFOA is significantly greater than TFOA.
Clinical presentation of knee OA and PFOA
What will your patient tell you? They’ll likely speak of morning stiffness, reduced range of motion, crepitus (an audible grinding noise and/or palpable vibrations), joint instability (the feeling of the knee giving-way), swelling, muscle weakness, fatigue, and pain, which are frequently observed in individuals with knee OA.
Peripheral nociceptive pain, neuropathic pain, or central pain mechanisms are also present in a large proportion of individuals with knee OA. Additionally, individuals who present with symptomatic PFOA will often complain of pain in and around the PF region during weight-bearing activities whilst the knee is flexed (such as during stair ambulation, squatting, and rising from sitting).
Of note is recent evidence highlighting the biomechanical similarities between patellofemoral pain (PFP) and PFOA. It has been proposed that individuals with prolonged or intermittent bouts of PFP may go on to develop PFOA, thereby forming a continuum of disease between the two conditions as seen in Figure 2.2-5 This is why it is important to ask your patient if they have previously experienced periods of anterior knee pain (AKP), even during their adolescent years.
Figure 2. Patellofemoral continuum (figured developed by Professor Kay Crossley with permission for reuse).
Diagnosis of knee OA and PFOA
They can both be diagnosed using:
Clinical signs and symptoms
Imaging features (such as joint space narrowing and osteophytes) from radiographs and/or MRI; or
A combination of clinical signs and symptoms and imaging findings.
Additional assessments which can assist with a clinical diagnosis of PFOA include:
Presence of crepitus (an audible grinding noise and/or palpable vibrations in the knee detected by the hand of the clinician rested on the patella of the patient while squatting)
Pain in and around the PF region whilst the patient undertakes weight-bearing activities whilst the knee is flexed (such as stair ambulation, squatting, rising from sitting)
A body mass index greater than 29kg/m2; AKP present for longer than 2.8 years; and inability to complete more than 21 single step-ups in a row before AKP sets in. However, it should be noted that further research regarding the diagnostic accuracy of PFOA is still required.
Foot and ankle and patellofemoral pathology
Patellofemoral OA is thought to be related to PF joint loading, with a number of factors having been associated with increased or abnormal PF joint loading. This results in an elevation of PF joint stress that, over time, causes a reduction in cartilage thickness and volume. In turn, this can facilitate OA development.
Static and dynamic foot and ankle characteristics that are thought to affect PFJ loads are shown in the table below:
Static and dynamic foot and ankle characteristics which may influence PFJ loads
Greater and lesser weight-bearing ankle joint dorsiflexion range (9, 10)
Arch Index (AI) – pes planus feet (11)
Greater Foot Posture Index (FPI) (12)
Greater/increased navicular drop (10, 12, 13)*
Greater navicular drift (10)
Greater midfoot mobility (9, 14)
Greater peak rearfoot eversion (15, 16)
Increased STJ pronation velocity (17)*
Lesser peak weight-bearing ankle joint dorsiflexion range (16)
*Denoted a risk factor for PFP development
Of the above foot and ankle characteristics, increased navicular drop13and increased STJ pronation velocity17are the two characteristics which have been shown to be risk factors (based on prospective study designs) for the development of PFP.
Interestingly, the relationship between weight-bearing ankle joint dorsiflexion range and PF pathology is inconsistent, with one study demonstrating less ankle joint dorsiflexion range16 and a second study demonstrating greater ankle joint dorsiflexion range10 when compared to healthy controls.
Despite the lack of longitudinal study designs investigating the pathomechanics of PF pathology, a small number of cross-sectional studies have demonstrated that the mechanics of the foot and ankle may influence PF joint loads, and therefore play a role in the pathogenesis and persistence of knee symptoms in these populations.
However, as static foot measures are not always associated with dynamic foot function18, this highlights the need to also include dynamic measures in an assessment of the foot and ankle. Once there is a clearer understanding of how foot and ankle function influences individuals with PFOA, effective interventions for this population can be further established and implemented.
Relatively few studies have investigated interventions for PFOA, and of the evidence available, the strength is somewhat limited.
The treatment options
Relatively few studies19-28 have investigated interventions for PFOA, and of the evidence available, the strength is somewhat limited. This makes the development and implementation of treatment plans for this population somewhat challenging.
Currently, limited evidence suggests that treatment for PFOA should include non-surgical and non-pharmacological interventions such as individualised physiotherapy, taping, or bracing. Furthermore, it is unknown if uni- versus multi-modal interventions improve outcomes in this population.
Of the successful interventions used to treat PFOA, the majority of interventions have been shown to be effective at reducing pain immediately 25, 28 or in the short (up to six weeks)24, 27, 27 to medium-term (two to six months)19, 23. Preliminary evidence suggests that foot orthoses may be effective immediately and into the medium-term23, 27, 28.
Currently, the long-term prognosis for individuals with PFOA using individualised physiotherapy, taping, bracing, or foot orthoses is unknown. The table below highlights interventions that have had their efficacy tested in individuals with PFOA.
Effective non-surgical interventions for reducing pain in PFOA
Immediately
Short-term (up to six-weeks)
Medium-term (two to six months)
Longer-term (seven months plus)
Foot orthoses28
Taping patella (medial direction)25
Foot orthoses27
Knee bracing49
Taping patella (medial direction)26
Foot orthoses23
Combined interventions (Physiotherapy: PFJ-targeted exercise, education, manual-therapy, and taping)19
Currently unknown – foot orthoses RCT data currently under analysis29
In summary
Knee OA and PFOA are highly prevalent conditions, with PFOA occurring in up to 43% of individuals who present with knee pain, and it is currently being observed in individuals as young as 26 years (post-ACLR).
Patellofemoral OA is also thought to form part of a continuum from PFP to PFOA and is a precursor to the development and progression of more extensive knee OA (such as TFOA/combined knee OA).
A thorough patient history and simple clinical assessments can assist with the clinical diagnosis of knee OA and PFOA without the need to refer on for imaging.
Altered foot and ankle characteristics (such as increased navicular drop and STJ pronation velocity) may impact PF joint loads and are possibly important in regards to the persistence of knee symptoms, development, and/or progression of PFOA.
Lastly, little research has investigated the effectiveness of treatments for PFOA in the immediate, short, medium and longer-term. However, preliminary evidence suggests that foot orthoses are effective in individuals with PFOA in the immediate, short, and medium-term, with data analysis currently underway regarding the longer-term effects of foot orthoses on pain in this population.
References
1Hunter DJ, Prieto-Alhambra D, Arden N. Osteoarthritis: The Facts. Oxford University Press, Oxford, 2014.
2 Wyndow N, Crossley KM, Hodges PW, Tsao H, Ozturk H, Hart HF, Vicenzino B, Collins N. Foot orthoses induce immediate changes in lower limb neuromotor control of gait in people with patellofemoral joint osteoarthritis: a pilot study. Osteoarthritis Cartilage 22: S119, 2014
3 Crossley KM, Hinman RS. The patellofemoral joint: the forgotten joint in knee osteoarthritis. Osteoarthritis Cartilage 19: 765, 2011
4 Thomas MJ, Wood L, Selfe J, Peat G. Anterior knee pain in younger adults as a precursor to subsequent patellofemoral osteoarthritis: a systematic review. BMC Musculoskelet Disord 11: 201, 2010
5 Conchie H, Clark D, Metcalfe A, Eldridge J, Whitehouse M. Adolescent knee pain and patellar dislocations are associated with patellofemoral osteoarthritis in adulthood: A case control study. Knee 23: 708, 2016
6 Powers CM, Maffucci R, Hampton S. Rearfoot posture in subjects with patellofemoral pain. J Orthop Sports Phys Ther 22: 155, 1995
7 Powers CM. The influence of altered lower-extremity kinematics on patellofemoral joint dysfunction: a theoretical perspective. J Orthop Sports Phys Ther 33: 639, 2003
8 Tiberio D. The effect of excessive subtalar joint pronation on patellofemoral mechanics: a theoretical model. J Orthop Sports Phys Ther 9: 160, 1987
9 Wyndow N, Collins NJ, Vicenzino B, Tucker K, Crossley KM. Foot and ankle characteristics and dynamic knee valgus in individuals with patellofemoral osteoarthritis. J Foot Ankle Res 11: 65, 2018
10 Mølgaard C, Rathleff MS, Simonsen O. Patellofemoral pain syndrome and its association with hip, ankle, and foot function in 16-to 18-year-old high school students: a single-blind case-control study. J Am Podiatr Med Assoc 101: 215, 2011
11 Gross KD, Felson DT, Niu J, Hunter DJ, Guermazi A, Roemer FW, Dufour AB, Gensure RH, Hannan MT. Association of flat feet with knee pain and cartilage damage in older adults. Arthritis Care Res 63: 937, 2011
12 Barton CJ, Bonanno D, Levinger P, Menz HB. Foot and Ankle Characteristics in Patellofemoral Pain Syndrome: A Case Control and Reliability Study. J Orthop Sports Phys Ther 40: 286, 2010
13 Boling MC, Padua DA, Marshall SW, Guskiewicz K, Pyne S, Beutler A. A prospective investigation of biomechanical risk factors for patellofemoral pain syndrome: the Joint Undertaking to Monitor and Prevent ACL Injury (JUMP-ACL) cohort. Am J Sports Med 37: 2108, 2009
14 McPoil TG, Vicenzino B, Cornwall MW. Effect of foot orthoses contour on pain perception in individuals with patellofemoral pain. J Am Podiatr Med Assoc 101: 7, 2011
15 Barton CJ, Levinger P, Crossley KM, Webster KE, Menz HB. The relationship between rearfoot, tibial and hip kinematics in individuals with patellofemoral pain syndrome. Clin Biomech 27: 702, 2012
16 Leitch J, Reilly K, Stebbins J, Zavatsky AB. Rear-foot kinematics in runners with PFPS during walking, squatting and uphill running. J Foot Ankle Res 5: P26, 2012
17 Hetsroni I, Finestone A, Milgrom C, Sira D, Nyska M, Radeva-Petrova D, Ayalon M. A prospective biomechanical study of the association between foot pronation and the incidence of anterior knee pain among military recruits. J Bone Joint Surg Br 88-B: 905, 2006
18 Paterson KL, Clark RA, Mullins A, Bryant AL, Mentiplay BF. Predicting dynamic foot function from static foot posture: comparison between visual assessment, motion analysis, and a commercially available depth camera. J Orthop Sports Phys Ther 45: 789, 2015
19 Crossley KM, Vicenzino B, Lentzos J, Schache AG, Pandy MG, Ozturk H, Hinman RS. Exercise, education, manual-therapy and taping compared to education for patellofemoral osteoarthritis: a blinded, randomised clinical trial. Osteoarthritis Cartilage 23: 1457, 2015
20 Hunter DJ, Harvey W, Gross KD, Felson D, McCree P, Li L, Hirko K, Zhang B, Bennell K. A randomized trial of patellofemoral bracing for treatment of patellofemoral osteoarthritis. Osteoarthritis Cartilage 19: 792, 2011
21 Quilty B, Tucker M, Campbell R, Dieppe P. Physiotherapy, including quadriceps exercises and patellar taping, for knee osteoarthritis with predominant patello-femoral joint involvement: randomized controlled trial. J Rheumatol 30: 1311, 2003
22 Eshnazarov K, Seon J, Song E. Comparison of Radiological Assessments Patellar Resurfacing with Retention for Grade IV Osteoarthritis in Patellofemoral Joint accomplished Total Knee Arthroplasty. Vestn Rentgenol Radiol 97: 28, 2016
23 Wyndow N, Crossley KM, Vicenzino B, Tucker K, Collins NJ. Footwear and custom foot orthoses versus footwear alone in individuals with patellofemoral joint osteoarthritis: a phase II randomized controlled pilot trial. Arthritis Care Res Accepted manuscript, 2019
24 Callaghan MJ, Parkes MJ, Hutchinson CE, Gait AD, Forsythe LM, Marjanovic EJ, Lunt M, Felson DT. A randomised trial of a brace for patellofemoral osteoarthritis targeting knee pain and bone marrow lesions. Ann Rheum Dis 74: 1164, 2015
25 Crossley KM, Marino GP, Macilquham MD, Schache AG, Hinman RS. Can patellar tape reduce the patellar malalignment and pain associated with patellofemoral osteoarthritis? Arthritis Care Res 61: 1719, 2009
26 Cushnaghan J, McCarthy C, Dieppe P. Taping the patella medially: a new treatment for osteoarthritis of the knee joint? Br Med J 308: 753, 1994
27 Tan JM, Menz HB, Crossley KM, Munteanu SE, Hart HF, Middleton KJ, Smith AJ, Collins NJ. The efficacy of foot orthoses in individuals with patellofemoral osteoarthritis: a randomised feasibility trial. Pilot Feasibility Stud 5: 90, 2019
28 Collins NJ, Hinman RS, Menz HB, Crossley KM. Immediate effects of foot orthoses on pain during functional tasks in people with patellofemoral osteoarthritis: A cross-over, proof-of-concept study. Knee 24: 76, 2017
29 Collins NJ, Tan JM, Menz HB, Russell TG, Smith AJ, Vicenzino B, Munteanu SE, Hinman RS, Haines TP, Hart HF, Patterson BE, Cleary G, Donnar JW, Maclachlan LR, Crossley KM. The FOOTPATH Study: protocol for a multicentre, participant- and assessor-blind, parallel group randomised clinical trial of foot orthoses for patellofemoral osteoarthritis. BMJ Open 9: 14, 2019